VENTANILLA - CALLAO (PERÚ)
Telefax.511. 553.0981. E-mail. lebr7@yahoo.com

VENTANILLA - CALLAO (PERÚ) |
|
|
| •
Página principal • Indice de productos |
• Venta
de productos • Páginas peruanas |
• Venta
de Maquinarias • Revistas en texto completo |
• Más
Monografias • ENLACES |
|
Bienvenid@s a La Página Virtual de ALNICOLSA del Perú S.A.C. Telf: 5530981 - Ultima Actualización |
Wounds
13(4):144-158, 2001. © 2001 Health Management Publications, Inc
The
use of tannic acid in the local treatment of burns is controversial. Although
it became the therapy of choice shortly after its introduction in 1925 and
most clinicians agreed upon its effectiveness, the tanning method was
generally abandoned again halfway through the forties, as hepatotoxic effects
were observed in both patients and experimental animals. However, a critical
evaluation of early literature data shows that hepatic necrosis and impairment
of liver function were not exclusively related to tannic acid treatment but
also occurred in patients who were treated otherwise. Moreover, in those
studies reporting adverse effects, tannic acid preparations of ill definition
and poor quality were used often in extremely high concentrations. More
recently, it has also become apparent that native pathophysiological
phenomena, rather than tannic acid intoxication, underlie the liver damage
seen in thermal injury. In this perspective, it is not surprising that the use
of tannic acid as an adjuvant therapy for burn wounds has regained interest in
present times. In particular, some preclinical and clinical studies indicate
that highly purified tannic acids can provide a valuable tool to improve wound
healing and to reduce scar tissue formation.
A
whole array of remedies has served in the local treatment of burns through the
ages. In ancient Chinese texts, many decoctions of medicinal herbs were
advocated for the "dispersal of heat and detoxication" of "fire
poison."[1] Similarly, the Ayurveda contains references to the
topical application to burn wounds of vegetable oils, powdered plant
materials, honey, or mixtures thereof.[2] In his presidential
address at the annual meeting of the American Burn Association in 1971,
Moncrief[3] presented an overview of the developments in topical
treatment of burns in the Western world. On this occasion, he recounted some
noteworthy early milestones, such as: Hippocrates' recommendation to use
swine's fat; the introduction in the 18th century of "Carron oil," a
popular therapeutic containing linseed oil and lime water that continued to be
used for over 200 years; and the appearance of boric lint and medicated
paraffin at the end of the 19th and the beginning of the 20th century.
Furthermore, Moncrief mentioned some recent progressions in this field through
chemical escharotics and antibiotic agents, such as the aniline dyes,
sulfonamide drugs, and penicillin, to eventually the adoption in burn therapy
of silver sulfadiazine. The latter compound, together with cerium nitrate,
which became available some years later,[4] has remained the
topical treatment of choice until now.
The
availability of increasingly adequate local therapeutics, in addition to
advances in general care of burn patients and improved surgical techniques,
have resulted in a gradual decrease of mortality due to burns. The work of
Davidson[5] in the 1920s laid the foundation for this development,
as it revolutionized the attitude of the medical profession toward the
treatment of burns and was the impetus for further research in this field. He
was one of the first who took pity on extensively burned patients and showed
that their terrible suffering may be alleviated by better local therapeutic
regimens, such as his tannic acid method of treatment. This method, which
became immensely popular shortly after its introduction and has recently
experienced a revival in interest, is the subject of this paper. The original
method applied by Davidson as well as all later modifications will be
reviewed. The arguments for and against the use of tannic acid, but in
particular its alleged hepatotoxic effects, will also be elaborated upon and
put in a historical perspective.
Tannins
comprise a large group of natural products widely distributed in the plant
kingdom. They have a great structural diversity, but in general, two classes
are distinguished, the hydrolyzable type and the condensed type.[6]
Hydrolyzable tannins are esters of sugars, mainly glucose, and phenol
carboxylic acids, such as gallic acid, hexahydroxydiphenic acid, or its stable
dilactone ellagic acid. As their name infers, hydrolyzable tannins are readily
degraded under hydrolytic conditions into these fundamental components.
Hydrolyzable tannins are present in many different plant species but are found
in particularly high concentrations in nutgalls growing on Rhus semialata
(Chinese and Korean gallotannins) and Quercus infectoria (Aleppo or
Turkish gallotannins), the seedpods of Caesalpinia
spinosa (Tara
tannins), and the fruits of Terminalia chebula.[7] The
condensed tannins are much more resistant to decomposition and merely yield
polymers or amorphous precipitates under the influence of acids. The basic
monomer of condensed tannins is (epi)catechin, which is extended by the
successive addition of similar units to form oligomers and polymers.
Traditionally, important commercial sources of condensed tannins are the
heartwood of Schinopsis lorentzii and S. balansae (Quebracho
tannins), the bark and/or heartwood of Acacia catechu (Catechu tannins)
and A. mollisima (Wattle or Mimosa tannins), and the bark of Rhizophora
and Eucalyptus species.[8,9]
Although
both types of tannin
have been used to treat diseases in traditional medicine, the hydrolyzable
tannins are generally considered as officinal in Europe and North America.
They have been included in many pharmacopoeias, in the older editions in
particular, and are specifically referred to as "acidum tannicum" or
tannic acid.[10-13] Few accounts with respect to the use of
condensed tannins originate from China, where plant extracts containing these
tannins as their major constituents are also applied as medicinal agents for
the treatment of burns.[14-16]
Incidental
accounts on the use of tannins and tannin-containing
plants can be found here and there in the history of burn treatment. However,
it is Davidson[5] who deserves the credit for introducing the
tannic acid method of treatment that became the standard therapy for burn
patients in subsequent years. It is his contribution to have developed one of
the first therapies that significantly improved the treatment of thermal
injury. The rationale behind Davidson's work was found in the toxin theory,
one of the many theories that had by then evolved to explain the diverse
pathophysiological phenomena observed in burn patients. This theory attributed
the systemic reactions seen in these patients to the absorption of some toxic
substance from the affected skin. It was, at that time, prevalent and most
strongly supported by experimental evidence. Thus, already in 1905, Pfeifer[17]
had reported the presence of a labile neurotoxic substance in the urine and
serum of experimentally burned mice. This toxin was also found to induce
necrosis of internal organs, in particular those of the gastrointestinal
tract. Pfeiffer's observations were confirmed by many others, perhaps most
convincingly by Robertson and Boyd in 1923.[18] These investigators
grafted burned skin onto normal animals, which showed toxic manifestations
within short notice. Likewise, injection of blood from burned animals into
controls resulted in toxic effects in the latter. They isolated and
characterized the toxin and found it to be composed of autolytic products of
decomposed proteins. These experiments convinced Davidson of the necessity to
prevent resorption of burn toxins into the circulation. To accomplish this
objective, he used tannic acid, since it has the property to complex with all
kinds of biomolecules and therefore "might be efficacious in
precipitating poisonous materials in burned tissue."[5]
In his
first publication on the subject, Davidson reviewed 25 case histories of burn
patients treated with tannic acid. After some initial experiments with
unfavorable outcomes in which he applied boric acid compresses to the tanned
eschar in an attempt to remove it, Davidson successfully employed the open
treatment method. Upon admission of the patient to the hospital, the burn
wounds were dressed with sterile gauze and bandages and moistened with freshly
prepared 2.5- to 5-percent aqueous solutions of tannic acid. The dressings
were kept wet until a satisfactory coagulum had been formed, and the wounds
had become insensitive to pain. At that moment, they were removed, and the
burns were exposed to air. In few cases, in particular in facial burns, a
5-percent ointment with a petrolatum and lanolin base was used instead of the
aqueous solutions.
In
Davidson's experience, tannic acid was best suitable in the management of
burns. It was superior to other therapeutic regimens, since it notably reduced
the degree of toxemia as determined from clinical and physico-chemical
observations and the lowered mortality rate. Tannic acid was also found to be
advantageous in several other respects. The local protein-precipitating
effects of tannic acid include relieving the pain, preventing the loss of
plasma, and markedly limiting secondary infection. Furthermore, in nonfatal
cases, a diminution in the amount of scar tissue formation was observed. This
was believed to be an additional effect of the formed coagulum, which could
provide "a scaffold for the growth of the young epithelial cells over the
denuded surface."[5]
The
tannic acid treatment of burns was adopted by many other clinicians, but in
actual practice, only a few strictly adhered to Davidson's original method.[19]
In the hands of others, it was soon modified to yield simpler or more
efficacious treatment procedures. Beck and Powers[20] sprayed the
burn frequently with a 2.5-percent aqueous solution until the wound surface
was tanned. This became the standard method of treatment and was widely
employed, although the concentrations of tannic acid used were liable to vary
and ranged from 2 to 20 percent.[21-28] Other ways to apply tannic
acid were also advocated, e.g., solved in physiological salt or Ringer's
solution instead of water,[29] in the form of gels and/or
ointments,[21,24,30-32] or as a bath.[33,34] Moreover,
the use of a diverse array of additives was proposed. Hunt and Scott[35]
used mixtures of tannic acid and collodion to strengthen the crust formed over
the burn wound. To speed up the tanning process, Bettman[36,37]
applied a 10-percent silver nitrate solution to the burn immediately after
treatment with tannic acid. For protection against infection, antiseptics,
such as perchloride of mercury,[25,26] dettol,[38]
gentian violet,[28,30] acriflavine,[27,28] salicylic
acid,[29] amyl-tricresol,[39] or
hexyl-dichloro-resorcinol[31,32] were sometimes added.
These
changes did not appear to influence the efficacy of tannic acid treatment, as
the results in general remained satisfactory and confirmed those of Davidson.
In agreement with Davidson, many authors stated that the use of tannic acid
was a distinct advance in the treatment of cutaneous burns and found the care
of patients relatively simple, since there was no longer distress from
dressing changes. Similarly, based on clinical experience, they almost
unanimously agreed upon such beneficial effects as rapid alleviation of pain,
lessened infection, reduced local loss of body fluids, prosperous
epithelization, relative absence of contractures, and diminished scar-tissue
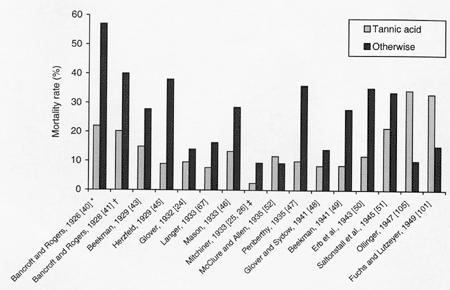
formation. But perhaps most important of all, good survival statistics were
reported in several studies (Figure). Thus, in 1926, one year after the
introduction of the tanning method, Bancroft and Rogers[40]
observed a reduction in the number of deaths in patients treated with tannic
acid in comparison to patients who had undergone debridement or were treated
with an electric cradle; mortality rates were 22, 57, and 50 percent,
respectively. Only patients treated by means of boric acid, picric acid,
sodium carbonate, or magnesium sulfate, alone or in combination, had a lower
mortality rate of 10 percent, but these were cases with burns of small total
body surface areas requiring little therapy. In a follow-up study with 114
patients by the same authors, these preliminary findings could be confirmed.[41]
In a series of 50 patients, Wilson[42] found the total number of
death to be seven, of which only four (8%) were directly attributable to the
injury. According to the author, this figure compared favorably with any that
had been quoted from other methods.
In a group of 114 patients treated with tannic acid, Beekman[43]
observed a mortality rate of 14.9 percent, which was considerably lower than
the death rate of 27.8 percent in the 320 patients treated otherwise. He also
showed that the number of patients dying from the second to the tenth day, the
period of toxemia, was strongly decreased in the tannic acid-treated group.
Likewise, Davidson and Penberthy44 mentioned a drop in mortality in the period
after thermal insult that was generally associated with the toxemic phase.
Moreover, the results of nearly all studies carried out in subsequent years,
up to the early forties, paralleled these initial observations.[24-26,45-51]
In one publication only, an increase in the incidence of death after tannic
acid treatment was noted, although this was no reason for the authors to
reject this method since, as it was stated, it had numerous distinct
advantages.[52]
|
|
|
Figure.
|
Comparative
mortality rates of tannic acid and other methods of burn treatment as mentioned in the
literature. Note that in many instances only a limited number of patients were
available to establish the mortality rates, and those patients did not always
represent uniformly distributed populations with respect to the severity of
the burn injury or age. This is best exemplified by quoting Ollinger[105]
who stated that "for the proper evaluation of the high mortality rate in
the tannic acid-treated burn patients it is essential to keep in mind that
merely the most severe cases were treated with tannic acid, a group which
would anyhow have shown the highest number of death." Some authors used
several alternatives for tannic acid. In those cases where no overall
mortality rates could be calculated,[25,26,40,41] bars depict only
one other treatment method: * debridement; † picric acid and dry air; ‡
picric acid (1924-1928). For the study by Fuchs and Lutzeyer,[101]
a mean mortality rate of four different treatment regimens is depicted. The
mortality rate of single alternative methods
was, in some cases, much higher. Thus, the number of deaths in
sulfonamide-treated children was identical to that of tannic acid-treated
children.
The
application of tannic acid to burn wounds has not been restricted to North
America and the United Kingdom. Its effectiveness was also recognized in
several other countries, such as France,[53] Spain,[54]
Romania,[55] The Netherlands,[56] and Denmark.[57]
However, in German-speaking countries in particular, many studies were
performed to rate this new treatment regimen at its true value and to compare
it with the current local therapy at that time of cod-liver oil.[58]
With just one exception, which was a trial with severely burned patients of
whom it was doubtful whether they would have survived or not under normal
treatment,[59] the outcome of those studies were in line with the
Anglo-Saxon literature data. Patients did clinically well,[60-66]
and a reduction in mortality was observed.[67,68] It is striking to
note that in most cases, these positive effects were obtained with Davidson's
original method that was quite strictly adhered to. The only major
modification that was propagated was the use of tannic acid ointments on a
basis of glycerine,[66,69] lanolin, and petrolatum-based ointment[68,70,71]
or other fatty oils.[72]
The
tannic acid method was widely met with enthusiasm, and it came to assume a
dominating position in the treatment of burn patients. Notwithstanding, this
method could not satisfy all needs and had its limitations and disadvantages
as may be expected in the case of an injury that was so difficult to treat and
often demanded all of the clinician's skills to arrive at a positive outcome.
First,
critics pointed out that this local therapeutic regimen did not consider
specific measures to improve the general conditions of patients. The
significance of such a systemic treatment, in particular fluid administration,
had just become apparent with the work of Underhill and co-workers[73]
and Blalock.[74] These authors demonstrated that the marked
concentration of blood and lowering of blood pressure were due to the local
loss of fluids and favored the suggestion that symptoms encountered in
severely burned patients were due to this fluid loss rather than to the action
of burn toxins.[75] Although from both clinical (vide supra) and
experimental data[76,77] it could have been concluded that tanning
may also improve the general condition of the patient by reducing the leakage
of plasma from burn wounds, it was nevertheless feared that focusing mainly on
the local treatment may incur the risk of distracting the attention from other
systemic measures that could be beneficial to the patient's welfare.[78]
In this respect, it was even suggested that the observed drop in the mortality
rate could not be solely attributed to the introduction of tannic acid
treatment but should, at least in part, be ascribed to the simultaneous
advances in the general care of burn patients.[49,50,52,72,79,80]
Second,
it was considered inappropriate by some to apply tannic acid to burns of the
hands and face.[81-83] When used on the hands, tannic acid would
form an inelastic eschar and prevent transudation, which could lead to edema
formation, compression of the circulation, and finally necrosis of fingers or
deformities of the hand. Tanning of facial burns may be detrimental in that,
with the multiplicity of orifices in the vicinity, it was almost impossible to
avoid infection. It could furthermore immobilize the eyelids, which may result
in dehydration of the eyes and, consequently, inflammation and eventual loss
of sight.
Third,
it was put forward that tannic acid may destroy intact epithelium and in this
way could inflict further damage, so that in some instances a second-degree
burn is converted into a third-degree burn. With respect to this objection,
considerable evidence both for and against has accumulated. In support of the
belief that tannic acid damages epithelial cells, Taylor[79] noted
that the viable epithelium stopped abruptly where the coagulum began. Ham[77]
found a considerable thickness of dermis to be destroyed but only when the
burned surface was denuded of epidermis prior to tanning. Similarly, Hirshfeld
and associates[84] reported that in fresh wounds resulting from
skin grafting, the dermis was destroyed to a great depth after application of
tannic acid. The same authors observed a delay in epithelial regeneration and
prolonged healing time, a finding that was confirmed by others.[80,83,85]
The cause for these adverse effects on skin structure is not known exactly but
might be related to the high acidity of the solutions[86] or the
type of tannic acid used.[87] Opposed to this, a substantial body
of evidence is available to refute the opinion that tannic acid is detrimental
to epithelium. From the clinic, many reports on the prosperous healing of burn
wounds have been issued (vide supra). In addition, Bancroft and Rogers,[40]
looking into more detail to this aspect, found healthy skin to be apparently
unaffected by tannic acid treatment. In microscopic examination of biopsies
taken from one case, they also saw a thin layer of flat epithelium extending
from the hair follicle and spreading out over the connective tissue. Likewise,
Baltin[66] found the hair follicles and glands from which
reepithelization may occur to be well preserved. Anagnostidis[88]
did not observe any differences between tannic acid-treated and untreated burn
wounds with respect to the microscopic wound characteristics and the healing
process. Finally, Von Löhr and Zacher[58] examined the ability of
tannic acid to fixate dead tissue in experimental burn wounds in animals and
human operation material and showed the coagulating effect to be only
superficial.
Fourth,
the poor antibacterial capacity was assumed to be another negative aspect
because it brought with it the risk of infections to spread under the eschar,
thereby inducing further tissue damage.[58,82,83,89] The picture of
heavily infected burn patients with profuse discharges and dressings soaked
with odorous and often green pus was sometimes referred to as the
"laudable pus days"[52] and was generally seen before the
introduction of tannic acid treatment. This, however, was rarely encountered,
though local foci of infection remained common. Thus, it was noted that in
third-degree burns, there are a certain number of patients who develop
infection,[41,85] and it was demonstrated that bacteria, in
particular Streptococci, were present in burn wounds.[38,90] The
insufficiency of tannic acid to prevent infection became particularly evident
during the Second World War. While it was advocated by the Royal Navy as a
first aid measure[91] and was considered to be the proper therapy
in superficial burns by other war surgeons,[82,92] in more
unfavorable situations it was far from adequate. For example, Porritt[93]
reporting on the desert wars in the Middle East during the "Wavell,"
"Auchinleck," and "Alexander-Montgomery" periods found
tanning in forward areas near the war front to be depressing in the extreme:
Nine out of ten patients arrived in the hospital septic and in very poor
general condition, and all that could be done for them was to remove the
septic eschar. However, it should be noted that these battle casualty burns
were, more frequently than not, serious and usually combined with other
wounds, and transportation to the hospitals took, in general, several days or
even more than a week. To overcome this particular problem of infection,
several authors suggested the use of combined preparations of tannic acid and
antiseptics (vide supra) or advocated the use of coagulating agents other than
tannic acid, such as gentian violet, which had similar protein-precipitating
properties but was a more potent bactericidal.[90]
However,
none of these drawbacks associated with the use of tannic acid gave cause to
reconsider its use on burn wounds. They were merely the reason for slight
changes in the formulation or adaptations in the method of application. It was
not until the late thirties and beginning of the forties, after reports on the
potential hepatotoxic effects of tannic acid started to appear, that the
opinion concerning the value of tannic acid treatment underwent a dramatic
change.
In
1938, Wilson, MacGregor, and Stewart[28] were the first to report
on the occurrence of liver lesions in tannic acid-treated burn patients.
Post-mortem examination in a series of 33 severely burned, fatal cases
revealed a characteristic degeneration and necrosis of liver cells, which was
much more intense than that seen in other organs. In its mildest form, it
appeared as a fatty degeneration of the epithelial cells surrounding the veins
in the central zone of the hepatic lobules but could, in more advanced
examples, progress to a total destruction of the central zones in which only a
narrow strip surrounding each portal tract showed surviving liver cells. In
subsequent years, several other communications were published describing liver
damage in burn patients who had some form of tannic acid therapy. Buis and
Hartman[32] confirmed the findings by Wilson, et al.,[28]
and, in addition, noted that the lesions in humans were identical to those
found in experimentally burned animals treated with tannic acid jelly. Belt[94]
reported histopathological changes that closely resembled those of yellow
fever. McClure,[78] McClure and Lam,[31] and Duffin[95]
observed the clinical signs of a marked jaundice and decreased liver function
accompanied by central liver necrosis in some patients who failed to survive.
Evidence of an impaired liver function has also been reported by others.
Wolff, Elkinton and Rhoads,[96] as well as Abbott and Holden[97]
found an elevation of blood bilirubin, impairment of glycogenesis and hippuric
acid synthesis, and a decrease in prothrombin levels. However, none of these
authors associated the phenomena seen in burn patients with the application of
tannic acid but merely suggested it to be a consequence of toxemia and the
circulation of burn toxins.
Only in
1942, Wells, Humphrey, and Coll[34] directly related the occurrence
of liver damage to the tannic acid therapy. In their article in the New
England Journal of Medicine, these authors described four patients who
died three to five days after the injury, in the period which was generally
associated with toxemia. In agreement with previous observations, on autopsy
these patients exhibited central lobular liver necrosis as the outstanding
feature or as the sole cause of death. Since the common denominator appeared
to be the employment of tannic acid in these cases, the possible role of this
constituent in the production of hepatic damage was further investigated. For
this purpose, a series of experiments was performed in which rats were
subcutaneously injected with different doses of tannic acid. This induced
liver damage that was essentially similar to the lesions in humans and was
proportional to the amount of tannic acid administered. Therefore, it was
concluded that the liver damage seen in burn patients might be due to tannic
acid poisoning and that it should be distinguished from the patient's toxemic
phase, which resulted from the resorption of toxins from the burn wound.[34]
Following
the experiments by Wells and coworkers, additional evidence was accumulated
for the detrimental effects of tannic acid. The occurrence of hepatotoxic
signs in tannic acid-treated burn patients was confirmed by several other
clinicians.[50,51,98-102] The hepatotoxic signs were also related
to the increase in the frequency of liver necrosis seen in fatal burns[103,104]
and the comparable higher mortality rates as found in some late clinical
trials (Figure 1).[101,105] Also, experimental data from animal
studies provided further support for its harmfulness. Subcutaneous injection
of tannic acid gave a disturbed liver function[106,107] and a
fairly uniform and specific liver necrosis.[108-111] Intramuscular
injections resulted in a slight, though definite, liver damage.[112]
Intravenous injections produced severe liver lesions in mice[109,112]
and more variable pathological changes in rabbits.[106] When tannic
acid was applied to denuded skin surfaces, the amount of liver damage seemed
to be dependent on the application form and the type of animal. An aqueous
solution or an ointment usually produced hepatic necrosis in rats, whereas no
lesions could be found when tannic acid was combined with silver nitrate.[108]
Dogs treated with tannic acid jelly showed congestion, fatty degeneration, and
myelinization of the liver but no central necrosis.[111]
Application of tannic acid to denuded surfaces was lethal for mice but not for
rats or rabbits.[107] Neither was liver damage, as measured by the
Bromsulphalein test, seen in rabbits.[107] A comparable variation
in the degree of liver damage was found when tannic acid was applied to
experimentally induced burns. In guinea pigs there was only slight liver
damage,[112] and burned dogs showed clinical jaundice and central
liver necrosis in just a limited number of cases.[111] Conversely,
varying degrees of liver damage were observed in goats and rabbits, although
this was in no case as severe as after subcutaneous injection.[109]
As
a consequence of these clinical and experimental observations, it became the
dominating view for many years that deaths of liver necrosis were due to
tannic acid; eventually, tannic acid treatment was generally abandoned.
However, a few clinicians remained advocates of this therapy, especially in
Germany.[113-117] In this country, the modest revival in interest
in the use of tannic acid as an adjuvant therapy in the treatment of thermal
injury started. It was first reintroduced in the early eighties by Hettich
from Tübingen-University. By using a three-phased tanning procedure
consisting of the subsequent application of solutions of Mercurochrome or
iodine-povidone, tannic acid, and silver nitrate, he was able to conserve the
burn wound and to delay primary excision.[118,119] This method had
various advantages; the principle was that surgical debridement of the burned
surface could be postponed and performed when the patient recovered from the
first consequences related to the trauma. In addition, since second-degree
burns were spontaneously reepithelized, less grafting material was needed, and
if necessary, the newly formed epithelium could be used as autograft for large
skin defects.
Subsequently,
following Hettich's example, the application of tannic acid to burn wounds was
resumed in some tentative studies in the Burn Centre of the Red Cross Hospital
in Beverwijk, The Netherlands. Here tannic acid was no longer considered as
the topical therapy of first choice, since newly available drugs, such as
silver sulfadiazine and cerium nitrate, were better suitable in this respect,
but it was valued for its potential superior long-term wound healing
characteristics. The first indications for the beneficial effects on wound
healing and scar tissue formation were obtained from animal experimental work.
In a comparative burn wound model in the Yorkshire pig for the
histopathological evaluation of local therapeutic regimens, tannic acid
ointment was found to induce a durable, supple crust that did not obstruct the
regular outgrowth of epithelium. Macroscopically, a striking diminution of the
hyperemic zone was observed. Tannic acid-treated burns also showed fewer
inflammatory signs as was established by microscopic investigations.[120,121]
Further research provided evidence that tannic acid could be combined with
other topical agents currently used in the clinic. Thus, combination with
silver sulfadiazine in an alternating mode did not influence the physical
qualities of the crust and resulted in a similar decrease of fibrosis and
fibrovascular reactions in the wound bed.[122] In agreement with
this, in a recent laboratory study, it was established that silver and cerium
ions did not negatively interfere with the collagen cross-linking ability of
tannic acid.[123]
The
positive effects as seen in these experimental settings could be confirmed in
a clinical trial with a limited number of patients. When applied to burn
wounds after standard debridement and disinfection, tannic acid induced a
supple crust within three days after the start of treatment, which remained
intact for one to four weeks, depending on the area of the body treated and
the involvement of joint regions. The wound healing was undisturbed, and no
deepening of the burns was observed. In comparison with the universal silver
sulfadiazine cream treatment, tannic acid-treated wounds demonstrated
remarkably little granulation tissue.[124] Healed areas were
covered with an epithelium with normal aspect, and the remaining scar was
supple and not abnormally vulnerable. In seven out of nine patients, no
hypertrophic scar formation was found, whereas in the other two patients, the
hypertrophic area amounted to not more than 10 percent of the original tannic
acid-treated region.[125]
Native
pathophysiological phenomena, rather than tannic acid intoxication, induce the
hepatic lesions seen in burn injury. In particular, the many clinical and
experimental observations made in the forties were indicative for a potential
hepatotoxic effect of tannic acid. Consequently, in general, this method of
burn treatment is still considered as obsolete, although it has become
apparent in the meantime that it might be beneficial when used as an additive
therapeutic regimen under strictly controlled conditions. However, the assumed
hepatotoxicity of tannic acid can be questioned when those early publications
are analyzed in retrospect and with the knowledge acquired in recent years
kept in mind.
For
instance, references to pathological hepatic changes and impairment of liver
function in burn patients are not restricted to the episode in which tannic
acid therapy was widespread. Although not specifically emphasized as a
characteristic feature, liver damage was already reported in papers that
appeared prior to the introduction of tannic acid treatment. As early as 1898,
Bardeen[126] reviewed in detail the lesions found at post-mortem
examination in some fatal burn cases. Macroscopically, the chief gross change
was a swelling of the liver. Microscopically, he noticed a parenchymatous
swelling of the epithelium with focal areas in which there was marked
vacuolization of the cell nucleus and some nuclear fragmentation, as well as a
moderate congestion and capillary thrombosis. Likewise, Vogt[127]
observed a fatty degeneration of liver epithelial cells and Kupffer cells
along with an accumulation and degradation of white blood cells in the liver
capillaries in burn patients who had died before 1925. Weiskotten[128]
found no constant changes to be evident in the liver on gross examination, but
microscopically he could detect foci of liver cell necrosis in two out of ten
patients. Signs of liver injury were also mentioned by many authors during the
tannic acid era in patients who were treated otherwise as well as shortly
after cessation of local treatment with tannic acid. Reports on fatty changes,
congestion and edema, and several forms of liver degeneration are relatively
common.[50,103,104,129] Although possibly occurring less frequent,
hepatic necrosis was observed in those patients as well. Zinck[130]
found necrosis to occur in five out of twelve patients. Extensive burns
involving approximately half of the total body surface, which led to a quick
death, produced most striking damage to the central and intermediate parts of
the hepatic lobules in this series of patients.[130] Baker[131]
noted minimal degrees of necrosis to be present in four cases in which the
burn itself may have been the cause. Moderate to severe necrosis, extending to
more than a quarter or nearly one-half of the distance from the central vein
to the periphery of the hepatic lobules, respectively, was also observed, but
this was attributed to complications of the burns or other accessory factors,
such as thrombosis and infection.[131] In addition, some degree of
liver dysfunction in burn patients who were not treated with tannic acid could
often be established by laboratory tests. Patients treated with gentian violet
showed marked deviations from the normal in the dextrose tolerance test.[96,132]
These alterations in liver function were comparable to those seen in tannic
acid-treated patients.[96] Abnormalities in the serum bilirubin
levels, the Bromsulphalein retention test, the hippuric acid conjugation test,
and the cephalin flocculation test were shown after treatment with coagulating
agents other than tannic acid or petrolatum gauze, with or without pressure
dressing.[51] Using essentially similar test systems, James and
coworkers[133] obtained comparable results. Furthermore, changes
that were indicative for liver necrosis were found in the urine of burn
patients treated with cod-liver ointment, indifferent ointment, or sterile
dressings only.[101,102]
Similar
to the results of human studies, histopathological and functional changes of
the liver have been observed following experimentally induced thermal injuries
in animals that did not receive tannic acid treatment. Thus, different levels
of liver damage, ranging from serous inflammation, turbid distension,
dissociation to fatty and parenchymatous degeneration, and even necrosis, were
found in histological examinations in guinea pigs[114,115,134] and
rabbits.[17] Impairment of hepatic functioning, as detected by a
decreased clearance of the dye Rose Bengal, was also reported.[135]
Furthermore,
in those studies evaluating the effects of tannic acid on the liver, the
outcomes were not always univocal. The results obtained in at least two animal
studies were contradictory to the general perception that tannic acid is
hepatotoxic. Ahnefeld[114] noted a decrease in the incidence and
severity of liver damage in experimentally burned guinea pigs treated with
either a tannic acid spray or ointment in comparison with control animals. In
experiments by the same author in which tannic acid was applied to artificial
wounds after surgical removal of the skin, liver histology was essentially
normal as well.[114] More recently, it was shown by Schölmerich
and coworkers[136] that application of tannic acid to burned rats
prevented some changes in liver morphology and metabolism. Animals treated one
hour after burning showed no signs of ultrastructural changes in the liver
cells, and blood urea concentrations were only slightly lowered or reached
normal levels when animals were treated with tannic acid one hour or
twenty-four hours after induction of the injury, respectively.
Additionally,
it should be taken into account that the experimental design of those toxicity
studies where a harmful effect of tannic acid was seen did not or only partly
reflected clinical practice, which makes it difficult to extrapolate the
findings. This difficulty of applying observations in animals directly to the
human situation lies on the one hand in the differences in morphological and
functional skin characteristics. Therefore, perhaps with exception of the pig
model,[121] animal models for burn injury are, in general, not
strictly comparable to human burns. Neither are the various denudation
experiments[107,108,111] comparable in this respect. On the other
hand, the dosages administered to animals as well as the mode of application
of tannic acid also hampers comparison. The amounts of tannic acid given were
often very high and exceeded, by far, the concentrations of the solutions
applied on burn wounds. Likewise, absorption characteristics of subcutaneous,
intramuscular, or intravenous injections are completely different from a
topical administration to damaged skin.
However,
it is not only this substantial body of evidence accumulated in the past that
justifies the question of tannic acid being detrimental to the liver. Starting
in the early sixties, it was gradually realized that hepatic failure was
inextricably bound with the burn syndrome. The impetus for this change in the
way of thinking has certainly been the fact that adequate tests became
available to determine serum transaminase levels,[137] which
facilitated the noninvasive diagnosis of liver damage in the course of time.
With the aid of these enzyme assays, it was established that hepatocytes are
subject to destruction in burn patients[138-146] and in
experimentally burned animals.[147-153] Along with the results of
these enzyme tests, more data were collected on the histopathology of the
liver following thermal injury. At present, reports on different levels of
liver damage, ranging from fatty changes, congestion, and edema, and several
forms of liver degeneration to necrosis, are quite common.[117,141,147,150,153-157]
The
experiments by the group of Allgöwer and Schoenenberger from the University
of Basel in Switzerland have also been of significant importance in the
conception that native pathophysiological phenomena, rather than tannic acid
intoxication, underlie the liver damage seen in burn injuries. These
researchers isolated and characterized a toxic macromolecular lipid-protein
complex from burned mouse and human skin and from the serum of burn patients.[158-161]
In various studies, the effects of this toxic complex on structural and
metabolic parameters of the liver were extensively examined and compared with
those observed after a controlled in-vivo burn injury. Using
autoradiography, it was shown that 14C-labelled toxic complex accumulated in
practically all organs with a significant preference for the liver.[162]
Ultrastructural changes in the mitochondria of hepatocytes ranging from
cristolysis, partial intramitochondrial vacuolization, and sometimes a total
vacuolar destruction of mitochondria were found to occur both after toxin
injection and experimental burn. The specificity of these alterations was
proven by application of different doses of toxin, which resulted in a
dose-dependent increase in destruction.[163,164] This damage to the
mitochondria, where the cellular oxygenation chain is located, was reflected
in liver metabolism studies, which demonstrated that several processes
depending on ADP-rephosphorylation, such as gluconeogenesis, glycogen
synthesis, and urea formation, were inhibited.[165]
Finally,
it should be realized that the tannic acid preparations used in the thirties
and forties for the local treatment of burn patients and in the early toxicity
studies were ill defined and of low purity. This is reflected, in particular,
in the pharmacopoeia descriptions of medicinal tannic acid of those days. In
the Pharmacopoeia of the United States of America of 1926, it was
described as "a tannin
usually obtained from nutgall,"[13] not at all specifying the
plant material from which the galls originated. Other pharmacopoeia were more
explicit but still allowed various plant species to be used as a source of
tannic acid. In the British and French pharmacopoeia, Turkish or Aleppo galls
from several Quercus species were mentioned as sources of tannic acid.[10,12]
However, according to commentaries on the pharmacopoeia of Germany and
Switzerland, tannic acid may also be derived from Chinese or Korean galls
growing on R. semialata.[166,167] Likewise, the few reports
in which reference was made to the type of tannic acid indicated that no
unequivocal, well-characterized products were used in clinical and
experimental studies carried out from the 1920s to the 1940s. Thus, the use of
aleppo,[25,26] quebracho,[84] and catechu[87]
tannins was mentioned. These tannins are derived from different plant species
and, as is known today, vary considerably in composition; the latter two do
not even contain tannic acids in any strict sense as their major constituents
(i.e., galloyl-glucose esters) but rather condensed tannins.[168]
Just as there was a poor definition of the plant species from which tannic
acids were derived, original methods
used for isolation were also inadequate and merely consisted of simple solvent
extraction procedures. For instance, the extraction of tannic acid from
fermented plant galls with water-saturated ether is described in the British
Pharmacopoeia.[10] In particular, the purity, expressed as the
percentage of tannic acid, of the products obtained in this way was relatively
low. Thus, in two studies performed around 1930, the total tannic acid content
in several products, as estimated by the hide powder method, was found to
range from 55 to 90 percent depending on the extraction solvent and plant
material used.[169,170] More recently, it was shown by
high-pressure liquid chromatography and other analytical methods
that in a tannic acid sample from 1940 the content of galloyl-glucose esters
comprised only 35 percent of the total, in addition to high levels of other
constituents, such as condensed tannins, flavonoids, and gallic acid.[171]
Furthermore, the complexity of tannic acid products or tannin
extracts was not appreciated in this period, and it was not until the early
fifties, with the introduction of adequate separation techniques, that it
could be demonstrated that tannin
extracts in general consisted of a large number of different substances.[172,173]
It is reasonable to suspect this poor quality of the older tannic acid
preparations to have contributed to at least part of the detrimental effects
observed in burn patients and toxicity studies. In particular, the presence of
contaminants, such as gallic acid, which is a metabolite formed during the
breakdown of tannic acid, might have been disadvantageous in this respect.
Proof for this assumption was recently acquired in some experiments in which
it was shown that gallic acid, even when present in low concentrations,
completely blocked the protein-binding capacity of tannic acid preparations.[174]
Therefore, it is conceivable that gallic acid, but probably also other
impurities, may have hampered the fixation of endogenous burn toxins in the
skin, thereby constituting a potential hazard to the liver. The toxic effects
observed in several animal studies may be explained in a similar way.
Attenuation of the protein-binding capacity may have resulted in a higher
availability of unbound tannic acid, which consequently may have given rise to
an increase in bodily uptake and elevation of plasma concentrations.
In
summary, tannic acid can be considered as one of the more important
therapeutics used in the topical treatment of burn patients throughout the
20th century. Its use, however, changed dramatically over time, and many
positive reactions regarding the effectiveness were issued shortly after its
introduction by Davidson in 1925. However, the tannic acid method became
obsolete after the appearance of several reports on hepatotoxicity in the
early forties. Only in present times, with advances in the fields of burn
research, does a better understanding of the pathophysiology of the burn
syndrome, the involvement of the liver therein, and tannic acid research
occur. As a result, with the availability of highly purified tannic acids, the
usefulness of tannic acid as an adjuvant therapy has again gained interest.
This rise and fall in popularity of tannic acid is also reflected in review
articles that have been published over the years on this subject. Lee and
Rhoads in 194489 stated that tannic acid was applied successfully and, in
fact, had produced a decrease in mortality rate despite the occurrence of
liver necrosis. In subsequent reviews, the latter aspect was emphasized.[175-177]
Conversely, in 1995 Hupkens, et al.,[178] once more made the
necessary differentiations in the reports on hepatotoxicity of tannic acid and
reevaluated its use for better cosmetic results.
In this
respect, a parallel may be drawn between tannic acid and silver, another
therapeutic regimen for the local treatment of burns. After a period in which
the use of silver was reviled, it has again obtained an important place in the
contemporary treatment of burn wounds.[179,180] Similarly, as it
appears to be now, highly purified tannic acids might gain interest as a tool
to improve wound healing and to reduce scar tissue formation. However, prior
to the reintroduction of tannic acid in burn treatment, a thorough
benefit-risk analysis
should be carried out. This will, in the near future, require controlled
prospective studies comparing tannic acid with current standard therapeutic
regimens, such as the local application of silver sulfadiazine, with rigorous
toxicological assessment in which any detrimental effects of tannic acid on
the liver are to be excluded.
In
anticipation of such tests, it was attempted in this review to tentatively
answer the question of whether or not tannic acid actually is toxic to the
liver. From the collected data, it can be concluded that the evidence yet is
inconclusive. Thus, many clinical and experimental studies in the past were
indicative for a potential hepatotoxic effect of tannic acid. However, tannic
acid preparations of ill definition and poor quality were used, often in
extremely high concentrations. This could have negatively affected the outcome
of these studies. Moreover, liver damage and impairment of liver function also
occurred in patients who did not receive tannic acid treatment at all, and
these phenomena are now considered part of the burn syndrome. On basis of
these considerations, the suggestion by some that tannic acid has been a
contributing factor to the death among burn patients seems to be untenable,
also in light of the lowered mortality rate found in most clinical studies. It
is our opinion that the local application of tannic acid to burn wounds causes
no serious hepatic damage, at least not any more than the thermal injury does
in itself. A prerequisite is that it is used under strictly controlled
conditions, that a highly purified tannic acid product is applied in moderate
concentrations (at maximum 2.5- to 5-percent tannic acid), and an adequate
pharmaceutical formulation is used, which minimizes decomposition and creates
a favorable environment for wound healing.
The
library staff of Utrecht University is acknowledged for all their efforts to
retrieve relevant articles. This study is financially supported by the
foundation Achmea Slachtoffer en Samenleving, Zeist, The Netherlands.
Hsu
WS. Traditional Chinese treatment of burns. In: Yang CC, Hsu WS, Shih TS
(eds). Treatment of Burns. Berlin, Germany: Springer, Verlag,
1982:140-50.
Central
Council for Research in Indian Medicine and Homoeopathy. Handbook of
Domestic Medicine and Common Ayurvedic Remedies. New Delhi, India: Ministry of Health and Family Welfare,
Government of India, 1978:41-2.
Moncrief JA. The development of topical therapy. J Trauma 1971;11(11):906-10.
Monafo WW, Tandon SN, Ayvazian VH, et al. Cerium
nitrate: A new topical antiseptic for extensive burns. Surgery
1976;80(4):465-73.
Davidson EC. Tannic acid in the treatment of burns. Surg Gynecol Obstet 1925;41:202-21.
Haslam
E. Practical Polyphenolics: From Structure to Molecular Recognition and
Physiological Action. Cambridge, UK: Cambridge University Press,
1998:10-83.
Mussche
R. Isolering, struktuurbepaling en industriële toepassingen van
hydrolyseerbare plantaardige looistoffen. Farm Tijdschr België
1989;66(1):2-6.
Gnamm
H. Die Gerbmittel; allgemeine Beschreibung der pflanzlichen Gerbmittel.
In: Bergmann M, Gnamm H, Vogel W (eds). Die Gerbung mit
Pflanzengerbstoffe; Gerbmittel und Gerbverfahren. Wien, Austria:
Verlag von Julius Springer, 1931:1-100.
Haslam
E. Chemistry of Vegetable Tannins. London, UK: Academic Press,
1966:14-65.
British
Pharmacopoeia.
Acidum tannicum [Acid. tann.], tannic acid. London, UK: Constable & Co
Ltd., 1932:32.
Deutsches
Arzneibuch.
Acidum tannicum - Gerbsäure. Berlin, Germany: R. v. Decker's Verlag,
1926:32-3.
Pharmacopée
Française, 6th edition. Tannin
officinale, acidum tannicum. Rennes, France: Imprimeries Oberthur,
1937:1017-9.
Pharmacopoeia
of the United States of America, 10th Decennial Revision.
Acidum tannicum, tannic acid. Philadelphia, PA: JB Lippincott Company,
1926:28-9.
Anonymous.
Studies on the toxic effects of certain burn escharotic herbs. Chinese
Med J 1978;4(5):388-93.
Yang
CC, Xiao YR, Li YY. Management of the burn wound. In: Yang CC, Hsu WS,
Shih TS (eds). Treatment of Burns. Berlin, Germany: Springer
Verlag, 1982:41-105.
Shi
TS. Use of combined traditional Chinese and western medicine in the
management of burns. Panminerva Med 1983;25(3):197-202.
Pfeiffer
H. Experimentelle Beiträge zur Ätiologie des primären
Verbrennungstodes. Virchows Arch Pathol Anat 1905;180(3):367-435.
Robertson
B, Boyd GL. Toxemia of severe superficial burns. J Lab Clin Med
1923;9:1-29.
Gordon
RM. Treatment of burns by tannic acid. Lancet 1928(Feb 18):336-7.
Beck
CS, Powers JH. Burns treated by tannic acid. Ann Surg 1926;84:19-36.
Fraser
J. The treatment of burns in children. BMJ 1927(June 18):1089-92.
Griffith
GC. The treatment of burns in the Presbyterian Hospital of Philadelphia. Int
Clinics 1928;4:129-31.
Montgomery AH. The tannic acid treatment of burns in children. Surg Gynecol Obstet 1929;48:277-80.
Glover DM. Six years of tannic acid treatment of burns. Surg Gynecol Obstet 1932;54:798-805.
Mitchiner
PH. Treatment of burns and scalds with special reference to the use of
tannic acid. BMJ 1933;(Mar 18):447-52.
Mitchiner
PH. Treatment of burns and scalds with special reference to the use of
tannic acid. Lancet 1933;(Feb 4):233-9.
Wilson
WC. Extensive burns and scalds. Edinburgh Med J 1935;42:177-92.
Wilson WC, Macgregor AR, Stewart CP. The clinical course and pathology of burns and scalds under modern methods of treatment. Br J Surg 1938;25:826-65.
Fantus B, Dyniewicz HA. Compound
solution of tannic acid. J Am Med Assoc 1937;109(3):200-3.
Heggie
JF, Heggie RM. Antiseptic analgesic tannic acid jelly for burns. Lancet
1940;(Sept 28):391.
McClure
RD, Lam CR. Problems in the treatment of burns; liver necrosis as a lethal
factor. Southern Surg 1940;9(4):223-34.
Buis
LJ, Hartman FW. Histopathology of the liver following superficial burns. Am
J Clin Pathol 1941;11:275-87.
Wells
DB. The aseptic tannic acid treatment of diffuse superficial burns. J
Am Med Assoc 1933;101:1136-8.
Wells
DB, Humphrey HD, Coll JJ. The relation of tannic acid to the liver
necrosis occurring in burns. New Engl J Med 1942;226(16):629-36.
Hunt
JH, Scott PG. The treatment of burns in out-patients with reinforced
tannic acid dressings. Lancet 1932;(Oct 8):774-6.
Bettman AG. Tannic acid and silver nitrate in burns. Surg Gynecol Obstet 1936;62:458-63.
Bettman
AG. The rationale of the tannic acid: Silver nitrate treatment of burns. J
Am Med Assoc 1937;108(18):1490-4.
Clark
AM, Cruickshank R. Observations on the treatment of burns. Lancet
1935;(Jan 26):201-4.
Hartman
FW, Schelling V. Effect of acids on certain carbocyclic antiseptics. Proc
Soc Exp Bio Med 1935;33:460-7.
Bancroft
FW, Rogers CS. The treatment of cutaneous burns. Ann Surg
1926;84(1):1-18.
Bancroft
FW, Rogers CS. Late treatment of burns. Arch Surg
1928;16(5):979-99.
Wilson
WC. Treatment of burns and scalds by tannic acid. BMJ 1928;(July
21):91-4.
Beekman
F. Tannic acid treatment of burns, end-results in one hundred and fourteen
cases compared with three hundred and twenty treated by other methods.
Arch Surg 1929;18:803-6.
Davidson
EC, Penberthy GC. The treatment of burns in children with tannic acid. Proc
Internat Postgrad Med Ass 1929;5:265-8.
Herzfeld
G. The treatment of burns and scalds by tannic acid. Practitioner
1929;122:106-11.
Mason
JB. An evaluation of the tannic acid treatment of burns. Ann Surg
1933;97(5):641-7.
Penberthy
GC. Tannic acid treatment of burns. J Michigan Med Soc
1935;34(1):1-4.
Glover
DM, Sydow AF. Fifteen years of the tannic acid method of burn treatment. Am
J Surg 1941;51:601-19.
Beekman
F. In: Discussion following Glover DM, Sydow AF. Fifteen years of the
tannic acid method of burn treatment. Am J Surg 1941;51:601-19.
Erb
IH, Morgan EM, Farmer AW. The pathology of burns. Ann Surg
1943;117:234-55.
Saltonstall
H, Walker J, Rhoads JE, Lee WE. The influence of local treatment of burns
on liver function. Ann Surg 1945;121(3):291-300.
McClure
RD, Allen CI. Davidson tannic acid treatment of burns, ten year results. Am
J Surg 1935;28:370-88.
Leriche R, Jung A. Du traitement des brulures par l'acide tannique. Lyon Chir 1933;30(2):177-9.
Dueńo FP. Nuevas ideas en el tratamiento de las quemaduras graves. Arch Med Cir Espec 1930;32(23):593-7.
Floresco A. Le traitement des brulures par l'acide tannique. Gaz Hop Civ Milit 1927;100(78):1281-5.
Van der Spek J. Over de behandeling van brandwonden met versch bereide waterige looizuuroplossingen. Nederlands Tijdschr Geneesk 1931;75:873-7.
Wollesen JM. Gerbsäurebehandlung von Verbrennungen. Chirurg 1936;8(18):732-40.
Von Löhr W, Zacher K. Zur Klinik und Pathologie von Verbrennungen 2. und 3. Grades. Zentralbl Chir 1939;66(1):5-24.
Schreiner K. Die Therapie der Verbrennungen. Wiener Klin Wochenschr 1930;43(28):871-6.
Klug W. Über Behandlung ausgedehnter Verbrennungen. Zeitschr ärzt Fortbildung 1931;28(9):278-81.
Seifert E. Die Tanninbehandlung der frischen Hautverbrennungen und ihre fehlerhafte Anwendungsweise. Zentralbl Chir 1933;60:1051-5.
Wienecke H. Zur Behandlung der Verbrennungen. Med Welt 1933;7:1643-4.
Siber. Die Behandlung grosser Verbrennungen mit und ohne Tannin. Verhandlungen Dtsch Ges Unfallheilk 1934;(Oct 12):110-2.
Liebig AM. Sitzungsberichte aus chirurgischen Gesellschaften. Zentralbl Chir 1937;45:2600-1.
Flörcken H. Die Behandlung der Kriegsverbrennungen. Chirurg 1940;12(4):89-92.
Baltin W. Tanninbehandlung der Verbrennungen aller Grade. Monatsschr Unfallheilk 1942;49:65-80.
Langer M. Ueber die Resultate der Tanninbehandlung bei Verbrennungen im Kindesalter. Wien Klin Wochenschr 1933;46(22):689-90.
Saegesser M. Die Behandlung der Verbrennungen. Chirurg 1940;12(23):708-11.
Fasal P. Versorgung und Behandlung von Brandwunden. Chirurg 1938;10(13):454-62.
Gymnich W. Die Gerbsäure, ein altes Mittel zur modernen Behandlung von Verbrennungen bei plötzlichen Unglücksfällen. Med Welt 1932;6(46):1646.
Saegesser M. Die Tanninsäurebehandlung der Verbrennungen. Schweiz Med Wochenschr 1932;1:117-8.
Hilgenfeldt O. Die Behandlung und die pathogenetischen Grundlagen der Verbrennungen. Erg Chir 1936;29:102-210.
Underhill FP, Carrington GL, Kapsinow R, Pack GT. Blood concentration changes in extensive superficial burns, and their significance for system treatment. Arch Int Med 1923;32:31-49.
Blalock A. Experimental shock (VII) The importance of the local loss of fluid in the production of the low blood pressure after burns. Arch Surg 1931;22:610-6.
Underhill FP, Kapsinow R. The alleged toxin of burned skin. J Lab Clin Med 1931;16:823-30.
McClure GS. Evaporation of water from superficial burns. Arch Surg 1936;32(5):747-55.
Ham AW. Experimental study of the tannic acid treatment of burns with particular reference to its effect on local fluid loss and healing. Ann Surg 1944;120(5):698-706.
McClure RD. The treatment of the patient with severe burns. J Am Med Assoc 1939;113(20):1808-12.
Taylor F. The misuse of tannic acid. J Am Med Assoc 1936;106(14):1144-6.
Cannon B, Cope O. Rate of epithelial regeneration, a clinical method of measurement, and the effect of various agents recommended in the treatment of burns. Ann Surg 1943;117(1):85-92.
McIndoe AH. In: Hunter JB, Willcox W, chairs. Discussion at the joint meeting of the sections of surgery and of therapeutics and pharmacology of the Royal Society of Medicine. Lancet 1940;(Nov 16):621-2.
Wakeley CPG. In: Hunter JB, Willcox W, chairs. Discussion at the joint meeting of the sections of surgery and of therapeutics and pharmacology of the Royal Society of Medicine. Lancet 1940;(Nov 16):621-2.
Mowlem R. The treatment of burns. Proc Royal Soc Med 1941;34:221-4.
Hirshfeld JW, Pilling MA, Maun ME. A comparison of the effects of tanning agents and of Vaseline gauze on fresh wounds of man. Surg Gynec Obstet 1943;76:556-61.
Clowes GHA, Lund CC, Levenson SM. The surface treatment of burns, a comparison of results of tannic acid, silver nitrate, triple dye, and Vaseline or boric ointment as surface treatment in 150 cases. Ann Surg 1943;118(5):761-79.
Seeger SJ. The hydrogen-ion concentration value of tannic acid solutions used in the treatment of burns. Surg Gynec Obstet 1932;55:455-63.
Ullmann K. Bemerkungen über die Bedeutung der Gerbsäurebehandlung für die tägliche Praxis und die Pathologie der schweren Verbrennungszustände. Wiener Klin Wochenschr 1933;46(47):1437-9.
Anagnostidis N. Histologische experimentelle Untersuchungen über die Wirkung einzelner örtlich angewandter Arzneimittel bei Verbrennungen dritten Grades. Dtsch Zeitschr Chir 1939;252:248-56.
Lee WE, Rhoads JE. The present status of the tannic acid method in the treatment of burns. J Am Med Assoc 1944;125(9):610-2.
Aldrich RH. The role of infection in burns, the theory and treatment with special reference to gentian violet. New Engl J Med 1933;208(6):299-309.
Mitchiner PH. Thoughts on four years of war surgery -- 1939 to 1943. BMJ 1944;(Jul 8):37-40.
Atkins HJB. The management of burns. BMJ 1942;(Jun 13):729-31.
Porritt AE. Military surgery in the 'Middle East'. Br J Surg 1944;31:208-21.
Belt TH. Liver necrosis following burns, simulating the lesions of yellow fever. J Pathol Bacteriol 1939;48(3):493-8.
Duffin JD. Liver necrosis following burns. Can Med Ass J 1942;47:138-9.
Wolff WA, Elkinton JR, Rhoads JE. Liver damage and dextrose tolerance in severe burns. Ann Surg 1940;112:158-60.
Abbott WE, Holden WD. Prothrombin test as a diagnostic and prognostic aid. Arch Surg 1942;45:261-71.
Jackson AV. Liver necrosis in burns treated with tannic acid. Med J Australia (Sydney) 1944;2:352-4.
McClure RD, Lam CR, Romence H. Tannic acid and the treatment of burns: An obsequy. Ann Surg 1944;120(3):387-405.
Rae SL, Wilkinson AW. Liver function after burns in childhood, changes in laevulose tolerance. Lancet 1944;(Mar 11):332-9.
Fuchs HK, Lutzeyer W. Behandlung von Verbrennungen mit metallischem Aluminium. Ärztl Wochenschr 1949;4(11/12):181-3.
Stör O. Die Verbrennungskrankheit und ihre Behandlung. Stuttgart, Germany: Ferdinand Enke Verlag, 1952:37-49.
Gillman J, Gillman T. Structure of the liver in fatal burns. S Afr J Med Sci 1948;13:169-81.
Sevitt S. Burns, Pathology and Therapeutic Applications. London, UK: Butterworth & Co. Ltd., 1957:298-308.
Ollinger P. Ist die Tanninbehandlung bei Verbrennungen schädlich? Chirurg 1947;17/18(14):629-35.
Clark EJ, Rossiter RJ. Liver function in rabbits after injection of tannic acid. Lancet 1943;(Aug 21):222-3.
Robinson HJ, Graessle OE. Toxicity of tannic acid. J Pharmacol Exp Ther 1943;77:63-9.
Baker RD, Handler P. Animal experiments with tannic acid, suggested by the tannic acid treatment of burns. Ann Surg 1943;118:417-26.
Cameron GR, Milton RF, Allen JW. Toxicity of tannic acid, an experimental investigation. Lancet 1943;(Aug 14):179-86.
Forbes JC, Evans EI. Tannic acid and liver necrosis. Surg Gynecol Obstet 1943;76:612-3.
Hartman FW, Romence HL. Liver necrosis in burns. Ann Surg 1943;118:402-16.
Barnes JM, Rossiter RJ. Toxicity of tannic acid. Lancet 1943;(Aug 21):218-22.
Lust F, Pfaundler M. Krankheiten des Kinderaltes, Ihre Erkennung und Behandlung in der Praxis. Berlin, Germany: Urban und Shwarzenberg, 1946:16-8.
Ahnefeld FW. Ist die Ablehnung der Tannintherapie bei Verbrennungen berechtigt? Monatsschr Unfallheilk 1954;57:207-15.
Weber E. Die Tanninbehandlung bei der Verbrennungskrankheit. Langenbecks Arch Klin Chir 1955;282:122-4.
Grob M, Stockmann M, Bettex M. Lehrbuch der Kinderchirurgie. Stuttgart, Germany: Georg Thieme Verlag,1957:629-33.
Göring G, Langer G, Koch W, Schröder H. Erfahrungen mit der Verschorfungs- und Koagulationsbehandlung bei Verbrennungen im Kinderalter. Brunsweicher Beitrage Klin Chir 1968;216:545-52.
Hettich R. Die verzögerte primäre Exzision von Verbrennungsdefekten nach Gerbungsbehandlung. Helv Chir Acta 1982;49:575-82.
Hettich R, Koslowski L. Frühbehandlung der Brandwunden. Langenbecks Arch Chir 1984;364:205-11.
Hoekstra MJ, Rogmans MP. Experimental burns in pigs for the evaluation of topical wound therapy. In: Harding KG, Leaper DL, Turner TD (eds). Proceedings of the 1st European Conference on Advances in Wound Management. London, UK: Macmillan Magazines Ltd., 1992:11-3.
Hoekstra MJ, Hupkens P, Dutrieux RP, et al. A comparative burn wound model in the New Yorkshire pig for the histopathological evaluation of local therapeutic regimens: Silver sulfadiazine cream as a standard. Br J Plast Surg 1993;46:585-9.
Hoekstra MJ, Dutrieux RP, Rogmans MP. Tannin ointment alternated with silver sulfadiazine 1% cream versus tannin ointment alternated with silver sulfadiazine 1% liquid. Pre-clinical investigation report. Beverwijk, The Netherlands: Burns Research Institute, 1992.
Heijmen FH, Du Pont JS, Middelkoop E, et al. Cross-linking of dermal sheep collagen with tannic acid. Biomaterials 1997;18:749-54.
Kreis RW, Vloemans AFPM. Tannin ointment. Clinical pilot trial report. Beverwijk: Burns Research Institute, 1992.
Hupkens P, Hoekstra MJ, Vloemans AFPM, Kreis RW. Tannin ointment, follow-up results, Clinical pilot trial report. Beverwijk, The Netherlands: Burns Research Institute, 1993.
Bardeen CR. A review of the pathology of superficial burns, with a contribution to our knowledge of the pathological changes in the organs in cases of rapidly fatal burns. Johns Hopkins Hosp Rep 1898;7:137-79.
Vogt W. Über histologische Befunde beim Verbrennungstode. Virchow's Arch Pathol Anat 1929;273:140-62.
Weiskotten HG. Histopathology of superficial burns. J Am Med Assoc 1919;72(4):259-61.
Brenner F. Geringgradige Verbrennung als Ursache schwerer Organveränderungen. Centralbl Allg Pathol Path Anat 1936;65(4):97-101.
Zinck KH. Pathologische Anatomie der Verbrennung, zugleich ein Beitrag zur Frage der Blutgewebsschranke und zur Morphologie der Eiweisszerfallsvergiftungen. Veröffentl Konstitutions Wehrpathol 1940;46:1-232.
Baker RD. The internal lesions in burns with special reference to the liver and to splenic nodules. Am J Pathol 1945;21:717-39.
Elkinton JR, Wolff WA, Lee WE. Plasma transfusion in the treatment of the fluid shift in severe burns. Ann Surg 1940;112(1):150-7.
James GW, Purnell OJ, Evans EI. The anemia of thermal injury. II. Studies of liver function. J Clin Invest 1951;30:191-9.
Blüthgen H. Beitrag zur Pathologie der Verbrennung. Frankfurt ZeitschrPathol 1943;58:85-118.
Gilmore JP, Fozzard HA. Liver function following thermal injury. Am J Physiol 1960;198(3):491-5.
Schölmerich J, Richter IE, Mastari H, et al. Zur therapeutischen Beeinflussbarkeit der Toxinresorption bei Hautverbrennungen; synthetischer Hautersatz oder Tanningerbung. Anaesthetist 1981;30:185-90.
Reitman S, Frankel S. A colorimetric method for the determination of serum glutamic oxalacetic acid and glutamic pyruvic transaminases. Am J Clin Pathol 1957;28:56-63.
Bocanegra M, Hinostroza F; Kefalides NA. Serum transaminase changes in severe burns. Ann Surg 1963;157(3):438-45.
Reichard H, Liljedahl SO, Birke G. Serum activity of ornithinecarbamoyl transferase and transaminases in severe burns. Acta Chir Scand 1963;126:45-52.
Chlumsk J, Vrabec R, Hyncík V, et al. Clinical manifestation of the impairment of the liver in the course of the burn disease. Acta Chir Plast 1973;15(4):238-46.
Czaja AJ, Rizzo TA, Smith WR, Pruitt BA. Acute liver disease after cutaneous thermal injury. J Trauma 1975;15(10):887-94.
Hiramatsu M, Izawa Y, Hagihara M, et al. Serum lipid peroxide levels of patients suffering from thermal injury. Burns 1984;11:111-6.
Chiarelli A. Abnormal transaminase levels in burned patients. Plast Reconstr Surg 1985;75(1):134-5.
Chiarelli A, Casadei A, Pornaro E, et al. Alanine and aspartate aminotransferase serum levels in burned patients: A long-term study. J Trauma 1987a;27(7):790-4.
Chiarelli A, Siliprandi L, Casadei A, et al. Aminotransferase changes in burned patients. Intensive Care Med 1987b;13:199-202.
Latha B, Ramakrishnan M, Jayaraman V, Babu M. Serum enzymatic changes modulated using trypsin: Chymotrypsin preparation during burn wounds in humans. Burns 1997;23(7/8):560-4.
Arturson G. Serum glutamic oxalacetic transaminase activity in experimental burns. Acta Chir Scand 1961;120:303-8.
Arturson G, Wallenius G. The hepatocellular origin of circulating enzymes in experimental burns. Acta Chir Scand 1963;126:34-44.
Spector AA, Pauli WA. Early changes in serum enzymes in the rat following burn trauma. J Appl Physiol 1963;18(4):818-20.
Ashur H, Ben-Hur N, Kuperman O, Eshchar Y. Liver dysfunction and immunological disturbances in the thermal burn injury. Burns 1979;6(3):160-4.
Nishigaki I, Hagihara M, Hiramatsu, et al. Effect of thermal injury on lipid peroxide levels of rat. Biochem Med 1980;24:185-9.
Carter EA, Kirkham SE, Udall JN, et al. Thermal injury and gastrointestinal function II: Evidence for the production of hepatic dysfunction in the rat following acute burn injury. J Burn Care Rehabil 1986;7(6):475-8.
Nishimura T, DeSerres S, et al. Gene expression and cytokine and enzyme activation in the liver after a burn injury. J Burn Care Rehabil 2000;21:135-41.
Arturson G. Pathophysiological aspects of the burn syndrome. Acta Chir 1961;Suppl 274:1-135.
Teplitz C. Pathology of burns. In: Artz CP, Moncrief JA (eds). The Treatment of Burns, Second Edition. Philadelphia, PA: WB Saunders Co., 1969:22-88.
Talaat SM, El-din Beheri G, Zaki MS, El-Bolkainy N. Prevention of early histopathological changes in the liver in extensive burns. Br J Plast Surg 1973;26:132-9.
Angela G, Marino G, Teich-Alasia S, et al. Histopathology of the liver in 187 patients with severe burns: A needle biopsy study. Bull Clin Rev Burn Inj 1984;1:44.
Schoenenberger GA, Bauer U, Cueni LB, et al. Physical, chemical and biological properties of a specific toxic lipid-protein complex formed in thermally altered mouse skin. Biochim Biophys Acta 1972;263:164-77.
Schoenenberger GA, Cueni LB, Bauer U, et al. Isolation and characterization of a toxic lipid-protein complex formed in mouse skin by controlled thermal energy: Comparison to an inactive precursor derived from thermally unexposed or native skin. Biochim Biophys Acta 1972;263:149-63.
Schoenenberger GA. Burn toxins isolated from mouse and human skin. Monogr Allergy 1975;9:72-139.
Wüst B. Isolierung, physikalisc-chemische Charakterisierung, Immunologie und biologische Eigenschaften eines spezifischen cutanen Verbrennungstoxins und dessen Vorstufe beim Menschen [dissertation]. Basel, Switzerland: Universität Basel, GTP-Verlag, 1977.
Schoenenberger GA, Allgöwer M, Kremer B, Städler K. Neue Gesichtspunkte zur Verbrennungskrankheit. Chirurg 1976;47:582-8.
Kremer B, Frenzel H, Schoelmerich J, et al. Vergleichende transmissions- und rasterelektronenmikroskopische Untersuchungen über Leberveränderungen bei Mäusen nach subletaler Hautverbrennung und intraperitonealer Injektion eines spezifischen cutanen Verbrennungstoxins. Langenbecks Arch Chir Suppl Chir Forum 1977;30:145-50.
Kremer B, Allgöwer M, Scheidegger AM, et al. Toxin-specific ultrastructural alterations of the mouse liver after burn injuries and the possibility of a specific antitoxic therapy. Scand J Plast Reconstr Surg 1979;13:217-22.
Schölmerich J, Kremer B, Richter IE, et al. Effect of cutaneous human or mouse burn toxin on the metabolic function of isolated liver cells. Scand J Plast Reconstr Surg 1979;13:223-30.
Anselmino O, Gilg E (eds). Kommentar zum Deutschen Arzneibuch 6. Ausgabe 1926. Berlin, Germany: Verlag von Julius Springer, 1928:160-6.
Käsermann H (ed). Kommentar zur Pharmacopoea Helvetica, fünfte Edition. Zürich, Switzerland: Selbstverlag des Schweizerisches Apotheker-Vereins, 1949:132-3.
Santappa M, Sundara Rao VS. Vegetable tannins, a review. J Sci Industrial Res 1982;41:705-18.
Chemnitius F. Zur Technik der Tanninfabrikation. J Prakt Chem 1927;117:83-96.
Vogel W. Die Verarbeitung der pflanzlichen Gerbmittel auf Extrakte. In: Bergmann M, Gnamm H, Vogel W (eds). Die Gerbung mit Pflanzengerbstoffe; Gerbmittel und Gerbverfahren. Wien, Austria: Verlag von Julius Springer, 1931:290-364.
De Keukeleire D, Van Peteghem C, Everaert E. Updating of ADI for tannic acid, based on results from recent research and improvement of the quality. Scientific report. Gent, Belgium: University of Gent, 1993.
Kirby KS, Knowles E, White T. Tannins, part II: The complex nature of vegetable tannin extracts. J Soc Leather Trades Chem 1951;35:338-45.
White T, Kirby KS, Knowles E. The complexity of tannin extract composition. J Soc Leather Trades Chem 1952;36:148-55.
Halkes SBA, du Pont JS, Hoekstra MJ, et al. Gallic acid reduces the protein-precipitating capacity of tannic-acid preparations. In: Proceedings of the International Congress and 48th Annual Meeting of the Society for Medicinal Plant Research (GA): Natural products research in the new millennium. Zürich, Switzerland: ETH, 2000:SL06.
Rosenquist H. The primary treatment of extensive burns. Acta Chir Scand 1947;95(Suppl 124):1-128.
Harkins HN. The treatment of burns and freezing. In: Lewis D, Walters W, Blalock A, et al. (eds). Lewis' Practice of Surgery, Volume 1. WF Prior Company Inc., 1955:1-177.
Cope O. The end of the tannic acid era. Harvard Med Alumn Bull 1992;65:17-9.
Hupkens P, Boxma H, Dokter J. Tannic acid as a topical agent in burns: Historical considerations and implications for new developments. Burns 1995;21(1):57-61.
Klasen HJ. Historical review of the use of silver in the treatment of burns. I. Early uses. Burns 2000;26:117-130.
Klasen HJ. A historical review of the use of silver in the treatment of burns. II. Renewed interest for silver. Burns
Funding Information
Supported by the foundation Achmea Slachtoffer en Samenleving, Zeist, The
Netherlands
COPYRIGHT
© 2000 - 2003
ALNICOLSA del Perú S.A.C.
Prohibida su
reproducción total o parcial, así como su traducción a cualquier idioma sin
autorización escrita de su titular
Reproduction in whole or in part, or translation without written permission is
prohibited. All rights reserved